STD Testing California
Los Angeles, San Francisco, SanDiego, Sacramento, San Jose, Oakland & more …


Comprehensive Epidemiological Assessment of Sexually Transmitted Infections in California (2014–2024)
Trends, Geographic Distribution, Determinants, Forecasts, and Strategic Interventions📈 California STI Snapshot (2024)
1. Executive Summary: The State of the Syndemic
California, the nation's most populous state with over 39 million residents, stands at a critical epidemiological crossroads in sexual health management. The decade spanning 2014 to 2024 witnessed a complex and alarming transformation in the STI landscape, characterized by the dramatic resurgence of bacterial sexually transmitted infections (STIs), the emergence of antibiotic resistance, persistent health inequities, and the devastating rise of preventable congenital infections.
Despite California's reputation for progressive public health policies and robust healthcare infrastructure, the state has experienced relentless increases in chlamydia, gonorrhea, and syphilis rates that mirror—and in some metrics exceed—national trends. While the COVID-19 pandemic introduced significant data artifacts and temporary disruptions to screening and treatment infrastructure between 2020-2021, the underlying trajectory of bacterial STI transmission has been predominantly upward, driven by a syndemic of intersecting social, behavioral, and biological factors including unprecedented rates of homelessness, methamphetamine use epidemics, healthcare access disparities, and structural inequities that disproportionately impact communities of color and LGBTQ+ populations.
Conversely, recent data provides cautious grounds for optimism. The introduction of novel biomedical interventions, specifically Doxycycline Post-Exposure Prophylaxis (Doxy-PEP), offers a promising horizon for STI prevention. Early surveillance data from San Francisco and other progressive jurisdictions indicates potential 30-40% declines in bacterial STIs among MSM and transgender populations who have adopted this intervention. Additionally, policy innovations such as Senate Bill 306, which mandates insurance coverage for at-home STI testing, represent important steps toward reducing structural barriers to screening and early treatment.
2. Longitudinal Epidemiology: A Decade in Review (2014–2024)
Understanding California's STI epidemic requires careful analysis of three distinct epidemiological phases that shaped the past decade. Each phase reflects different combinations of biological transmission dynamics, healthcare system capacity, public health interventions, and external shocks to the healthcare delivery system.
2.1 Phase I: The Pre-Pandemic Surge (2014–2019)
The period from 2014 to 2019 was characterized by relentless, year-over-year increases in all major reportable STIs. This sustained growth occurred despite existing public health infrastructure, screening programs, and prevention efforts, suggesting fundamental shifts in sexual network dynamics, screening patterns, and underlying risk behaviors.
Chlamydia Trajectory:
Chlamydia cases increased from 174,270 in 2014 to a pre-pandemic peak of 237,630 in 2019—a 36.4% increase over five years. This growth averaged approximately 12,700 additional cases annually. The "silent" nature of chlamydia, which produces no symptoms in approximately 70% of women and 50% of men, means that true prevalence likely far exceeds reported cases. Increases were particularly pronounced among adolescents and young adults aged 15-24, who accounted for approximately 62% of all diagnosed cases.
Gonorrhea Escalation:
Gonorrhea demonstrated even more dramatic growth, nearly doubling from 44,907 cases in 2014 to 80,599 in 2019—a 79.5% increase. This represented approximately 7,100 additional cases per year. The rise coincided with decreasing antibiotic susceptibility to previously effective treatments, raising serious concerns about the eventual emergence of untreatable gonorrhea. Unlike chlamydia, gonorrhea more frequently produces symptoms (particularly in men), suggesting that the increase reflected true transmission increases rather than merely enhanced detection.
Syphilis Resurgence:
Perhaps most concerning was the syphilis resurgence. Total syphilis cases (all stages) more than doubled from 11,519 in 2014 to 28,846 in 2019—a 150% increase. Primary and secondary (P&S) syphilis, representing the most infectious stages, increased from 3,855 to 8,237 cases over the same period. This represented a complete breakdown of containment strategies that had successfully controlled syphilis for decades. The resurgence was driven by multiple factors: increased transmission among MSM networks, growing methamphetamine use facilitating high-risk sexual behaviors, and spillover into heterosexual networks, particularly among women of childbearing age.
2.2 Phase II: The COVID-19 Disruption (2020)
The onset of the SARS-CoV-2 pandemic in March 2020 created unprecedented disruption to STI surveillance, screening, and treatment infrastructure. The resulting "dip" in reported cases was primarily a surveillance artifact rather than a true reduction in disease transmission—a critical distinction for understanding subsequent trends.
- Clinic Closures: Sexual health clinics, family planning centers, and student health services closed or severely restricted operations during lockdown periods
- Resource Diversion: Public health personnel, laboratory capacity, and contact tracing infrastructure were massively redirected to COVID-19 response
- Deferred Care: Routine wellness exams and asymptomatic screenings—where most chlamydia cases are detected—were cancelled or indefinitely postponed
- Testing Anxiety: Fear of COVID-19 exposure deterred individuals from seeking in-person medical care for non-emergent conditions
Reported chlamydia cases dropped 25.4% from 2019 to 2020, falling to 177,230 cases. However, gonorrhea and syphilis—which more frequently produce symptoms prompting care-seeking even during a pandemic—showed smaller declines or remained relatively stable. This differential pattern strongly suggests that asymptomatic infections continued to circulate undetected, creating a reservoir of untreated infections that would later fuel transmission when screening resumed.
2.3 Phase III: Post-Pandemic Resurgence and Recent Stabilization (2021–2024)
As healthcare access normalized through 2021-2022, STI case counts rebounded sharply, with several indicators reaching all-time historical highs before showing signs of stabilization in 2023-2024. This phase reflects both "catch-up" diagnosis of infections acquired during the pandemic period and continued active transmission.
The 2021 Peak and Subsequent Trends:
Gonorrhea cases surged to a decade-high of 90,801 in 2021, representing a 12.7% increase from the pre-pandemic 2019 levels. This suggested significant undetected transmission during 2020 combined with ongoing high incidence. However, recent provisional data for 2023-2024 reveals a potential inflection point. Gonorrhea cases declined to 67,869 in 2024, representing a 25.3% decrease from the 2021 peak. Similarly, primary and secondary syphilis cases dropped from 8,791 in 2021 to 4,149 in 2024—a remarkable 52.8% decline.
- Doxy-PEP Uptake: Widespread adoption of doxycycline post-exposure prophylaxis in San Francisco and other jurisdictions, particularly among MSM populations
- Renewed Public Health Focus: Restoration and enhancement of STI prevention programs following COVID-19 disruptions
- Behavior Change: Possible sustained reductions in partner numbers or increases in condom use in some populations
- Enhanced Screening and Treatment: Implementation of home testing programs and expedited partner therapy
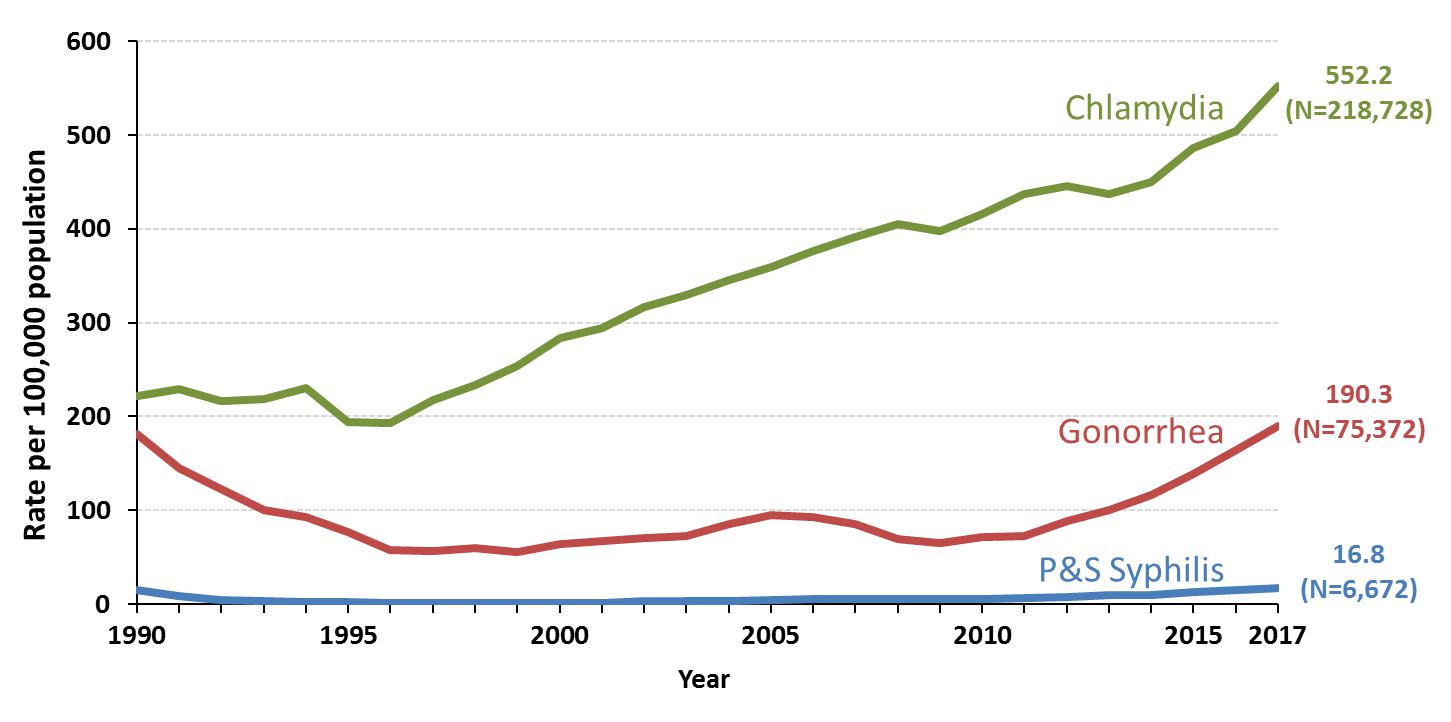
2.4 Comprehensive Data Visualization: Decade of Change
2.5 STI Rates Per 100,000 Population
3. Geographic Distribution: Regional Hotspots and Urban-Rural Disparities
California's STI epidemic is not uniformly distributed across the state's 58 counties. Instead, disease burden clusters in specific geographic areas shaped by population density, healthcare infrastructure, economic conditions, and demographic composition. Understanding these geographic patterns is essential for targeted intervention strategies.
3.1 High-Burden Urban Centers
The state's major metropolitan areas account for the vast majority of reported STI cases, reflecting both higher population density and more robust surveillance infrastructure. However, rates per capita reveal important disparities even among urban counties.
Population: ~815,000
Key Findings:
- Highest per-capita STI rates in California
- P&S syphilis rate: 65.8 per 100,000 (2023)
- 70% of syphilis cases among MSM
- Early Doxy-PEP adoption showing 30-40% decline in bacterial STIs (2023-2024)
- Concentration in Castro, Tenderloin, South of Market neighborhoods
Population: ~10 million
Key Findings:
- Largest absolute number of STI cases statewide
- 38,000+ gonorrhea cases annually (2023)
- Rising congenital syphilis: 180+ cases (2023)
- Severe disparities in South LA, East LA, and Long Beach
- High rates among unhoused populations (estimated 70,000+ experiencing homelessness)
Population: ~1.9 million
Key Findings:
- Emerging concern: Disseminated Gonococcal Infection (DGI) in adults 45+
- Tech industry demographics: high MSM population, delayed family formation
- 22 Mpox cases in 2024 (endemic persistence)
- Concentrated in San Jose, Palo Alto, Mountain View
Population: ~3.3 million
Key Findings:
- Major military presence: 18-25 age group disproportionately affected
- Border health considerations with Mexico
- Hillcrest/North Park: high MSM transmission
- Rising syphilis among women: 12.3 per 100,000 (2023)
Population: ~1.7 million
Key Findings:
- Oakland: severe racial disparities, 5x higher gonorrhea rates in Black communities
- Significant substance use overlap (fentanyl + meth epidemic)
- Public health infrastructure strained by homelessness crisis
Population: ~1.6 million
Key Findings:
- State capital: transient population, high mobility
- Documented syphilis outbreaks in 2022-2023
- Rural-urban interface: delayed diagnosis in suburban/exurban areas
3.2 Rural and Frontier Counties: Hidden Epidemics
While absolute case numbers are lower in rural California, per-capita rates can exceed urban areas due to limited healthcare access, stigma, poverty, and methamphetamine epidemics. Rural counties face unique challenges:
- Healthcare Deserts: Imperial, Inyo, Modoc, and other rural counties have few or no dedicated sexual health clinics
- Confidentiality Concerns: Small-town stigma deters testing; fear that providers know one's family or social network
- Economic Barriers: Long travel distances, time off work, lack of insurance
- Methamphetamine Crisis: Counties like Shasta, Kern, and Tulare see severe meth-STI syndemics
- Agricultural Workers: Migrant and seasonal farmworkers have limited healthcare access, language barriers, and fear of deportation
Counties of Concern:
- Fresno County: Central Valley agricultural hub; high rates among Latinx populations; congenital syphilis rates mirror urban areas
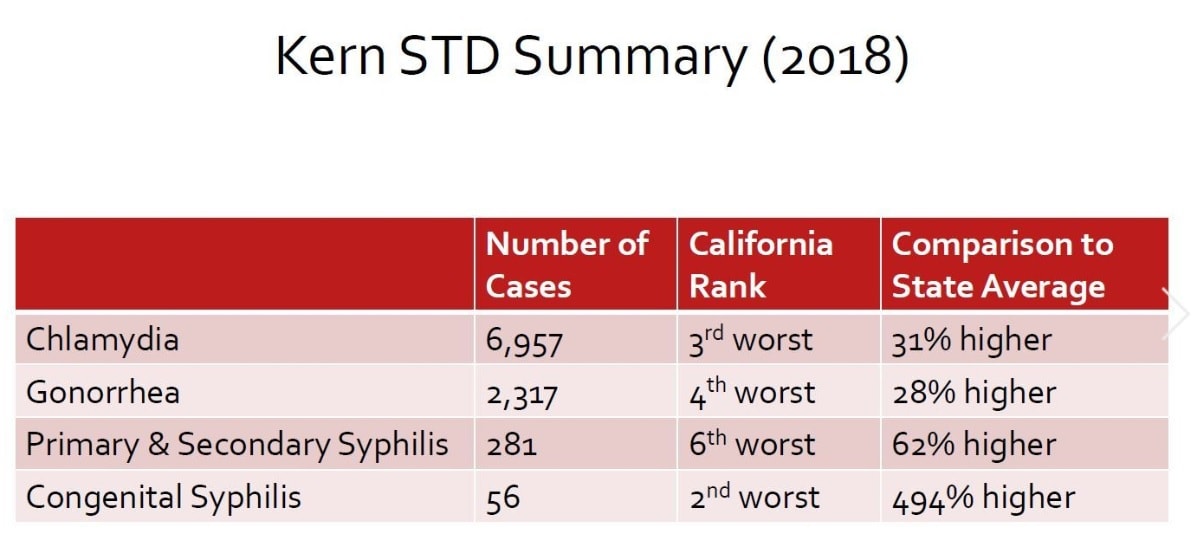
- Kern County (Bakersfield): Oil industry workforce; meth epidemic; gonorrhea rates comparable to Los Angeles on per-capita basis
- Imperial County: Border region; youngest median age in California; severe healthcare workforce shortages
- Humboldt County: Cannabis industry labor migration; high chlamydia rates among 15-24 age group
3.3 County-Level Case Distribution
4. Disease-Specific Analysis: Etiology, Trends, and Future Threats
4.1 Chlamydia trachomatis: The Silent, Persistent Reservoir
Chlamydia remains California's most prevalent reportable communicable disease, with 171,281 cases in 2024. Despite a decline from the 2019 peak, prevalence remains stubbornly high, reflecting the infection's insidious biology and the challenges of asymptomatic screening.
Clinical and Epidemiological Profile:
- Asymptomatic Reservoir: 70% of cervical infections and 50% of urethral infections produce no symptoms, allowing sustained community transmission
- Serious Sequelae: Untreated chlamydia causes Pelvic Inflammatory Disease (PID) in 10-15% of women, leading to chronic pelvic pain, ectopic pregnancy, and infertility. Men can develop epididymitis and reactive arthritis
- Age Distribution: 62% of cases occur in persons aged 15-24 years; highest rates in women aged 15-19 (3,300 per 100,000)
- Anatomic Sites: Rectal chlamydia in MSM often asymptomatic but facilitates HIV transmission; pharyngeal chlamydia rare but documented
Forecast for 2025-2030:
Expected Trajectory: Stabilization with potential artificial increases due to expanded screening access. As Senate Bill 306's home testing provisions reach full implementation, case detection will likely increase 10-15% in previously under-screened populations (young men, rural residents, uninsured individuals). True incidence may decline modestly if Doxy-PEP adoption expands beyond MSM populations.
- Extent of home testing uptake (could increase detection by 15,000+ cases)
- Doxy-PEP expansion to heterosexual populations (could reduce incidence by 8-12%)
- Restoration of school-based health center screening programs
4.2 Neisseria gonorrhoeae: Racing Against Resistance
While gonorrhea case counts have declined to 67,869 in 2024—the lowest since 2017—the primary public health threat is not current prevalence but the looming specter of untreatable, antibiotic-resistant gonorrhea.
The Antimicrobial Resistance Crisis:
Gonorrhea has demonstrated a remarkable ability to develop resistance to every antibiotic class deployed against it:
- 1940s-1970s: Sulfonamides and penicillin resistance emerged
- 1980s: Tetracycline resistance became widespread
- 1990s-2000s: Fluoroquinolone (ciprofloxacin) resistance forced removal from treatment guidelines
- 2010s-present: Rising cephalosporin resistance threatens last-line injectable ceftriaxone
International surveillance has detected alarming increases in reduced ceftriaxone susceptibility:
- UK: 0.8% resistant isolates (2022) → 5% (2024)
- Asia-Pacific: Multi-drug resistant strains documented in Japan, Australia
- California: Enhanced surveillance detected 3 cases of reduced susceptibility in 2023
Emerging Clinical Concern: Disseminated Gonococcal Infection (DGI)
Santa Clara County has documented unusual clusters of DGI—gonorrhea that spreads through the bloodstream to joints and other organs—particularly in adults over 45. DGI can cause septic arthritis, endocarditis, and meningitis. The reasons for this demographic shift are under investigation but may relate to delayed diagnosis in older adults who don't perceive themselves at risk.
Forecast for 2025-2030:
Optimistic Scenario: Continued Doxy-PEP expansion, aggressive contact tracing, and novel therapeutics (gepotidacin, zoliflodacin) prevent resistance crisis. Cases decline to 55,000-60,000 annually by 2030.
Pessimistic Scenario: Ceftriaxone-resistant strains become endemic. Without effective first-line treatment, gonorrhea cases surge to 100,000+ by 2028. Public health emergency declarations required; return to pre-antibiotic era management (long-term hospitalization for complicated cases).
4.3 Syphilis: A Tale of Two Epidemics
Syphilis in California represents two distinct, interconnected epidemics: one among MSM showing recent decline, and another among heterosexual populations—particularly women of childbearing age—driving a congenital syphilis catastrophe.
Primary & Secondary Syphilis in MSM:
San Francisco and other urban counties have documented 35-50% declines in P&S syphilis among MSM between 2021-2024, attributed to:
- High Doxy-PEP uptake (estimated 25-30% of sexually active MSM in San Francisco)
- Sustained HIV PrEP use (60-70% of at-risk MSM), which involves quarterly STI screening and treatment
- Targeted public health messaging and community engagement
Heterosexual Syphilis and the Congenital Crisis:
While MSM syphilis declines, syphilis among cisgender women has surged, creating a devastating cascade into congenital infections:
2024 Statistics: 438 cases of congenital syphilis in California
2014 Baseline: 104 cases
Increase: 321% over ten years
Consequences:
- 40% result in stillbirth or neonatal death
- Survivors face lifelong disabilities: blindness, deafness, skeletal deformities, neurodevelopmental delays
- Lifetime medical costs: $500,000-$2 million per affected child
Root Causes:
- Late or no prenatal care (75% of CS mothers had inadequate prenatal care)
- Methamphetamine use disorder (55% of CS mothers reported meth use)
- Homelessness and housing instability (48% of CS mothers unstably housed)
- Incarceration and criminal justice involvement
- Lack of partner treatment (65% of male partners not treated despite positive maternal test)
Neurosyphilis and Late-Stage Disease:
There are concerning reports of increasing neurosyphilis diagnoses, particularly among persons with HIV co-infection and those with delayed diagnosis. Neurosyphilis can cause dementia, stroke, blindness, and spinal cord deterioration. The rise may reflect both increased screening and true increases in late-stage, untreated infections.
Forecast for 2025-2030:
P&S Syphilis Overall: Continued decline to 3,000-3,500 annual cases by 2030 if Doxy-PEP expands and screening improves.
Congenital Syphilis: Without transformative intervention, CS will stabilize at 350-450 annual cases. Reduction requires:
- Universal first-trimester AND third-trimester screening (currently only 65% receive adequate screening)
- Street medicine programs providing syphilis testing and treatment to unhoused pregnant persons
- Mandatory partner notification and treatment
- Integration of substance use disorder treatment with prenatal care
4.4 HIV: Chronic Disease Management and Persistent Disparities
New HIV diagnoses in California have stabilized at approximately 4,100 annually (2022 data). The state has made remarkable progress toward UNAIDS 95-95-95 goals (95% diagnosed, 95% on treatment, 95% virally suppressed), but severe racial and geographic inequities persist.
Epidemiologic Shifts:
- Declining diagnoses among White MSM: PrEP uptake has dramatically reduced new infections in this demographic
- Persistent disparities among Black and Latinx MSM: Diagnosis rates 8-10x higher than White MSM, reflecting structural barriers to PrEP access
- Transgender women of color: HIV prevalence estimated at 28-44% in community-based studies—a humanitarian crisis that receives insufficient attention
- People who inject drugs: Small but concerning uptick in injection-associated transmissions, particularly related to fentanyl/stimulant co-use
PrEP Landscape:
Pre-Exposure Prophylaxis has been revolutionary but inequitably distributed. An estimated 180,000-200,000 Californians use PrEP, but this represents only 25-30% of those who could benefit. Barriers include:
- Cost and insurance barriers (improving with ACA mandates but still problematic for undocumented persons)
- Healthcare provider knowledge gaps in non-urban/non-MSM-focused practices
- Stigma and medical mistrust, particularly in communities of color
- Requirement for quarterly monitoring (lab visits, insurance authorization)
Forecast for 2025-2030:
Best Case: New diagnoses decline to 2,500-3,000 annually with:
- Long-acting injectable PrEP (cabotegravir, lenacapavir) reducing adherence barriers
- Targeted outreach to Black and Latinx communities
- Integration of PrEP into routine primary care
Concern: Racial disparities may persist or worsen if equity-focused interventions are not prioritized and funded.
4.5 Emerging and Under-Recognized Threats
Mpox (Monkeypox):
Following the explosive 2022 outbreak (5,000+ California cases), Mpox has settled into low-level endemicity with 50-100 annual cases statewide. The 2024 Santa Clara County data (22 cases) suggests continued transmission in sexual networks. The two-dose JYNNEOS vaccine provides 85% protection but uptake has plateaued at 40-50% of high-risk MSM. Ongoing concern exists for potential future outbreaks.
Mycoplasma genitalium:
This emerging STI is vastly under-recognized due to lack of routine testing. M. genitalium causes urethritis in men and cervicitis/PID in women, clinically indistinguishable from chlamydia and gonorrhea. Studies in sexual health clinics show:
- Prevalence: 10-16% of symptomatic STI clinic attendees
- Macrolide resistance: 40-50% of isolates (azithromycin ineffective)
- Fluoroquinolone resistance: Rising, approaching 10-15%
Without NAAT testing becoming standard, M. genitalium will remain a hidden driver of treatment failures and reproductive complications.
Lymphogranuloma Venereum (LGV):
LGV, caused by invasive serovars of Chlamydia trachomatis (L1, L2, L3), causes severe proctocolitis and systemic illness. Previously rare, LGV has emerged among MSM in urban centers, with outbreaks documented in San Francisco and Los Angeles. Diagnosis requires specialized testing; many cases are likely misdiagnosed as standard chlamydia and under-treated.
Hepatitis A, B, and C:
While technically not STIs, these viral hepatitides have significant sexual transmission components:
- Hepatitis A: Major outbreaks 2017-2020 among people experiencing homelessness and MSM; vaccination campaigns successful but waning immunity a concern
- Hepatitis B: Vaccine-preventable; declining due to universal infant vaccination but persistence among unvaccinated MSM and immigrants from endemic regions
- Hepatitis C: Rising among young people who inject drugs; new direct-acting antivirals are curative but expensive and under-utilized
5. Demographic Disparities: The Syndemic Landscape
STI burden in California is profoundly shaped by intersecting systems of oppression, structural inequities, and social determinants of health. Disease does not distribute randomly; it follows fault lines of racism, poverty, homophobia, and marginalization.
5.1 Racial and Ethnic Inequities
The STI epidemic in California reveals the ongoing legacy of structural racism, manifesting through residential segregation, educational inequities, economic disinvestment, mass incarceration, and discriminatory healthcare practices.
Black/African American Californians (6% of population):
- Chlamydia rate: 1,350 per 100,000 (vs. state average 540 per 100,000)
- Gonorrhea rate: 420 per 100,000 (vs. state average 190 per 100,000)
- P&S Syphilis rate: 38 per 100,000 (vs. state average 18 per 100,000)
- Black women aged 15-24: 500% higher chlamydia/gonorrhea rates than White women same age
Hispanic/Latinx Californians (39% of population):
- Largest absolute number of STI cases (110,000+ chlamydia cases annually)
- Congenital syphilis: 55% of all CS cases despite being 39% of population
- Highest rates in agricultural counties (Fresno, Kern, Tulare)
American Indian/Alaska Native:
- Chlamydia rates 2.1x state average
- Limited data due to small population but severe disparities documented
Asian American/Pacific Islander:
- Lowest reported rates BUT significant under-testing and cultural stigma suggest true rates higher
- Concerning increases in syphilis among API MSM in San Francisco, Los Angeles
Root Causes of Racial Disparities:
- Healthcare Access Barriers: Lack of insurance, underinsurance, provider shortages in communities of color, linguistic barriers, medical mistrust rooted in historical abuses (Tuskegee, forced sterilizations)
- Socioeconomic Factors: Poverty, unemployment, inability to take time off work for clinic visits, lack of transportation
- Mass Incarceration: Criminal justice involvement disrupts relationships, concentrates STI transmission, creates barriers to employment and housing post-release
- Sexual Network Dynamics: Racial residential segregation creates sexual networks within communities; if STI prevalence is high in a network, individual-level risk reduction has limited impact
5.2 Age: The Disproportionate Burden on Youth
Adolescents and young adults (ages 15-24) account for 47% of all new STIs despite being only 15% of California's population. This reflects both biological and behavioral vulnerabilities:
Biological Susceptibility:
- Cervical Ectopy: Adolescent females have larger areas of columnar epithelium on the ectocervix, which is more susceptible to chlamydia infection than mature squamous epithelium
- Immunological Naivety: Younger individuals may have less robust immune responses to initial STI exposures
Behavioral and Social Factors:
- Higher Partner Turnover: Shorter relationship duration, serial monogamy with brief gaps, overlap between partnerships
- Inconsistent Condom Use: Studies show only 25-30% of sexually active adolescents use condoms consistently
- Substance Use: Alcohol and marijuana use before sex associated with reduced protective behaviors
- Power Imbalances: Young women in relationships with older men may have less ability to negotiate condom use
- Healthcare Barriers: Concerns about confidentiality, parental notification, cost; lack of transportation; discomfort discussing sexual health
California's extensive higher education system (UC, CSU, community colleges, private universities) creates concentrated populations of sexually active young adults. Documented outbreaks include:
- UC Berkeley, UCLA, UCSB: Repeated chlamydia outbreaks 2018-2023
- SDSU: Meningococcal meningitis co-occurring with gonorrhea outbreak (2024)
- Student health centers overwhelmed; many students use commercial urgent care with inconsistent partner notification
5.3 Gender and Sexual Orientation: LGBTQ+ Populations
Men Who Have Sex with Men (MSM):
MSM continue to bear disproportionate STI burden while also demonstrating the highest responsiveness to biomedical and behavioral interventions:
- Syphilis: 70-75% of P&S syphilis cases occur among MSM
- HIV: 85% of new HIV diagnoses occur among MSM (despite being ~4-7% of male population)
- Rectal Gonorrhea/Chlamydia: Often asymptomatic; screening rates improving but still inadequate
- PrEP Success: Among MSM on PrEP with good adherence, HIV incidence has dropped >90%
- Doxy-PEP Impact: San Francisco MSM show 35-50% reductions in bacterial STIs within 12 months of adoption
Transgender Populations:
Transgender individuals face compounded vulnerabilities from discrimination, economic marginalization, healthcare exclusion, and violence:
- Transgender Women: HIV prevalence 28-44% in community-based studies (vs. <0.5% general population)
- Transgender Women of Color: Prevalence approaches 50-60% in some urban cohorts
- Transgender Men: Understudied but face barriers to cervical/anal screening due to provider discomfort, misgendering, lack of trans-competent care
- Survival Sex Work: Economic marginalization forces 30-40% into sex work at some point, increasing STI/HIV exposure
- Incarceration: Trans women often housed in men's facilities, experiencing high rates of sexual assault
Women Who Have Sex with Women (WSW):
Often mistakenly assumed to be at low STI risk, WSW can transmit bacterial vaginosis, trichomoniasis, and HSV through genital-genital contact, digital-vaginal contact, and shared sex toys. Healthcare providers frequently fail to screen WSW adequately.
Bisexual Individuals:
Bisexual persons may serve as "bridging populations" between higher-prevalence MSM networks and lower-prevalence heterosexual networks. They also face unique stigma ("bi-phobia") from both straight and gay communities, potentially reducing healthcare engagement.
5.4 Social Determinants: Housing, Substance Use, and Incarceration
Homelessness and Housing Instability:
California has the nation's largest population experiencing homelessness (>180,000 on any given night). Homelessness is perhaps the single strongest predictor of poor STI outcomes:
- Survival Sex: Trading sex for shelter, food, drugs
- Lack of Privacy: Sexual encounters in public spaces, encampments
- Competing Priorities: Sexual health screenings deprioritized when facing daily survival challenges
- Trauma and Mental Illness: High rates of PTSD, depression, psychosis reducing capacity for self-protective behaviors
- Poor Treatment Adherence: Inability to store medications, complete antibiotic courses; HIV viral suppression only 67% among unhoused PLWH (vs. 85% among housed)
Methamphetamine and Substance Use:
California faces a severe methamphetamine epidemic, intimately linked to STI transmission:
- "Party and Play" (PnP): Meth use in sexual contexts, particularly among MSM; marathon sexual sessions, multiple partners, reduced condom use
- Mechanism: Meth increases libido, delays orgasm, reduces pain perception (allowing rougher sex that tears mucosa and facilitates HIV/syphilis entry)
- HIV Risk: Meth use associated with 6-8 fold increased odds of HIV acquisition
- Congenital Syphilis: 55% of mothers of infants with CS report methamphetamine use
- Treatment Challenges: Meth use disorder complicates STI care; missed appointments, lost to follow-up for partner services
Criminal Justice Involvement:
Mass incarceration concentrates STI transmission and disrupts community sexual networks:
- High Prevalence: STI rates in California jails/prisons 3-5x general population
- Sexual Violence: Assault in detention facilities transmits HIV, syphilis, gonorrhea
- Reentry Challenges: Formerly incarcerated face barriers to housing, employment, healthcare; increased likelihood of unstable housing, transactional sex
- Partner Notification Disruption: Incarceration makes it difficult/impossible to notify and treat sexual partners
6. Strategic Interventions and Policy Solutions
6.1 Biomedical Innovations
Doxycycline Post-Exposure Prophylaxis (Doxy-PEP):
The most promising recent development in STI prevention, Doxy-PEP involves taking 200mg doxycycline within 72 hours of condomless sex. Evidence base:
- DoxyPEP Trial: 66% reduction in chlamydia, 55% reduction in syphilis among MSM/transgender women
- San Francisco Real-World Data: 30-40% decline in bacterial STIs among Doxy-PEP users (2023-2024)
- Mechanism: Bacteriostatic antibiotic inhibits protein synthesis in Chlamydia and Treponema pallidum; partial effect on Neisseria gonorrhoeae
Opportunities:
- Dramatic reductions in bacterial STIs possible with widespread uptake
- Self-administered, allowing user control
- Inexpensive generic medication
Challenges:
- Not recommended for cisgender women due to limited efficacy data
- Concerns about antibiotic resistance (though modeling suggests minimal impact if used correctly)
- Requires prescription access; insurance coverage variable
- Tetracycline photosensitivity and GI side effects
Long-Acting PrEP for HIV:
- Cabotegravir (Apretude): Injectable every 2 months; 70% more effective than oral PrEP; addresses adherence challenges
- Lenacapavir: Twice-yearly injectable under development; could revolutionize PrEP delivery
Future Vaccines:
- Gonorrhea Vaccine: Phase 2 trials of outer membrane vesicle vaccine showing promise
- Chlamydia Vaccine: Pre-clinical development; major challenge due to intracellular lifecycle
- HIV Vaccine: Renewed optimism with broadly neutralizing antibody approaches
6.2 Policy and Structural Interventions
Senate Bill 306 (2022):
Landmark legislation requiring health plans to cover at-home STI testing kits without cost-sharing. Implementation challenges include:
- Many insurers require provider prescription (barrier to access)
- Limited awareness among consumers and providers
- Self-collection kits may have lower sensitivity than provider-collected specimens for rectal/pharyngeal sites
Potential Impact: If fully implemented, could increase annual testing by 500,000-800,000 tests, particularly reaching young men and rural residents who avoid clinic-based care.
Congenital Syphilis Elimination Initiatives:
- Universal Third-Trimester Screening: Mandate syphilis testing at first prenatal visit AND in third trimester (currently recommended but not universally implemented)
- Street Medicine Programs: Mobile units providing prenatal care, syphilis testing, and penicillin treatment to unhoused pregnant persons in encampments
- Expedited Partner Therapy (EPT): Allow pregnant persons to carry medications home to treat partners without partner requiring separate visit
- Mandatory Reporting and Investigation: Treat every case of syphilis in a pregnant person as a public health emergency requiring immediate investigation and treatment
Decriminalization and Harm Reduction:
- Sex Work Decriminalization: Reduce barriers to healthcare for sex workers; eliminate fear of arrest when seeking STI services
- Syringe Services Programs: Expansion beyond opioids to include stimulant users; co-locate STI screening at syringe exchanges
- Housing First: Permanent supportive housing shown to improve HIV viral suppression, STI treatment completion
Healthcare System Reforms:
- Integrate STI Screening into Routine Care: Include STI panels in annual wellness exams; normalize sexual health discussions
- School-Based Health Centers: Expand confidential STI screening in high schools, community colleges
- Telehealth Expansion: Asynchronous telehealth for STI symptom evaluation, prescription of empiric treatment, home test kit prescription
- Provider Training: Mandatory LGBTQ+ cultural competency, trauma-informed care, antiracism training for all sexual health providers
6.3 Community-Level Interventions
- Peer Navigation Programs: Train community members (people living with HIV, formerly incarcerated, LGBTQ+ youth) as navigators to link high-risk individuals to services
- Social Marketing Campaigns: Culturally tailored messaging on social media, dating apps; normalize testing, reduce stigma
- Dating App Partnerships: Collaborate with Grindr, Tinder, etc. to send testing reminders, facilitate home test kit ordering, provide clinic locators
7. Forecasts and Future Scenarios (2025-2030)
7.1 Optimistic Scenario: "The Great Decline"
- Widespread Doxy-PEP adoption (40-50% of MSM, expansion to high-risk heterosexuals)
- Full implementation of SB 306 home testing
- Gonorrhea vaccine becomes available 2027-2028
- Sustained investment in congenital syphilis elimination
- Economic improvement, housing investments reduce homelessness 25%
2030 Projections:
- Chlamydia: 140,000-150,000 cases (12-18% decline from 2024)
- Gonorrhea: 45,000-50,000 cases (26-33% decline)
- P&S Syphilis: 2,500-3,000 cases (28-40% decline)
- Congenital Syphilis: 150-200 cases (54-66% decline)
- New HIV Diagnoses: 2,500-3,000 (30-40% decline)
7.2 Baseline Scenario: "Fragile Stability"
- Current trends continue; modest Doxy-PEP expansion
- Gonorrhea resistance remains <5%
- Homelessness crisis persists at current levels
- Some improvement in congenital syphilis from enhanced screening
2030 Projections:
- Chlamydia: 165,000-175,000 cases (stable to slight decline)
- Gonorrhea: 60,000-65,000 cases (stable to slight decline)
- P&S Syphilis: 3,500-4,000 cases (stable)
- Congenital Syphilis: 300-350 cases (modest decline)
- New HIV Diagnoses: 3,500-4,000 (stable)
7.3 Pessimistic Scenario: "The Resistance Crisis"
- Ceftriaxone-resistant gonorrhea becomes endemic (>10% resistance by 2027)
- Public health budget cuts reduce screening, contact tracing capacity
- Homelessness increases 30-40% due to housing costs, economic recession
- Doxy-PEP resistance emerges, reducing efficacy
2030 Projections:
- Chlamydia: 200,000-220,000 cases (17-28% increase)
- Gonorrhea: 95,000-110,000 cases (40-62% increase) - UNTREATABLE STRAINS CIRCULATING
- P&S Syphilis: 5,500-6,500 cases (33-57% increase)
- Congenital Syphilis: 550-650 cases (26-48% increase)
- New HIV Diagnoses: 5,000-6,000 (22-46% increase due to reduced PrEP access, increased untreated STIs facilitating transmission)
7.4 Comparative Forecast Visualization
8. Recommendations and Call to Action
For Policymakers:
- Increase STI prevention funding by 200% to match disease burden
- Mandate congenital syphilis elimination plans in all counties
- Expand Medi-Cal coverage for innovative prevention (Doxy-PEP, long-acting PrEP)
- Invest in permanent supportive housing (every $1 spent saves $2-3 in emergency healthcare)
For Healthcare Providers:
- Screen ALL sexually active patients annually (minimum)
- Ask ALL patients about sexual health without assumptions
- Prescribe Doxy-PEP to MSM/transgender patients at STI risk
- Implement third-trimester syphilis screening for ALL pregnant persons
For Individuals:
- Get tested regularly (at least annually if sexually active; every 3-6 months if MSM or multiple partners)
- Use condoms consistently or consider PrEP/Doxy-PEP if high risk
- Communicate openly with partners about testing, status
- Seek care immediately if symptoms develop
- Complete all antibiotic courses as prescribed
For Communities:
- Reduce stigma through education, normalization of sexual health discussions
- Support harm reduction services, syringe programs, housing initiatives
- Advocate for culturally competent, linguistically appropriate services
9. Conclusion: A Preventable Crisis Demands Action
The STI epidemic in California is not inevitable. Every infection represents a failure—of the healthcare system, of policy, of societal commitment to equity and dignity. Yet within this crisis lies profound opportunity. We possess the biomedical tools, the scientific knowledge, and the public health infrastructure to dramatically reduce STI burden. What we lack is political will, adequate resources, and societal commitment to prioritizing sexual health as fundamental to human dignity.
The 438 infants born with congenital syphilis in 2024 did not need to suffer. The thousands of young Black and Latinx Californians diagnosed with preventable infections did not need to face potential infertility, chronic pain, or lifelong HIV. The transgender women experiencing HIV prevalence rates comparable to generalized epidemics in sub-Saharan Africa deserve better.
California has led the nation in progressive health policy before—from tobacco control to HIV treatment as prevention. We can lead again on sexual health equity. The path forward requires transformative investments in housing, healthcare access, and harm reduction; rapid scale-up of proven biomedical interventions like Doxy-PEP and long-acting PrEP; elimination of structural barriers to care; and a fundamental reimagining of sexual health as a social justice and human rights imperative.
The data in this report should alarm us. But more importantly, it should mobilize us. Every Californian deserves access to comprehensive sexual health services. Every infant deserves to be born healthy. Every community deserves culturally responsive care. The time for incremental change has passed. The STI crisis demands—and our communities deserve—nothing less than transformative action.
The question is: WILL we?
Report compiled from California Department of Public Health surveillance data, CDC reports, peer-reviewed literature, and local health jurisdiction databases. Last updated: February 2025.