
Primary Stage of Syphilis: A Deep Dive into Symptoms and Mechanisms
Syphilis, caused by the bacterium Treponema pallidum, begins with a deceptively mild phase known as the primary stage. This stage is critical because it sets the foundation for the infection’s progression, yet its subtle symptoms often lead to delayed diagnosis. Below, we explore every facet of this stage, from initial infection to the body’s response, and why these manifestations occur.
Timeline and Initial Infection
After exposure (e.g., sexual contact), the bacteria enter the body through tiny cuts or mucous membranes. Here’s a timeline of events:
|
Timeline |
Key Events |
|
10–90 days post-exposure |
A painless sore (chancre) forms at the infection site (genitals, mouth, anus). |
|
3–6 weeks later |
The chancre heals on its own, but the infection persists and spreads silently. |
The primary stage typically starts 10 to 90 days after exposure, with an average incubation period of 21 days. The bacteria enter the body through microscopic breaks in the skin or mucous membranes during sexual contact. Once inside, T. pallidum uses its spiral shape and corkscrew-like motility to burrow into tissues, avoiding immediate detection.
The first visible sign is a chancre, a small, painless ulcer that forms at the infection site—commonly the genitals, anus, or mouth.





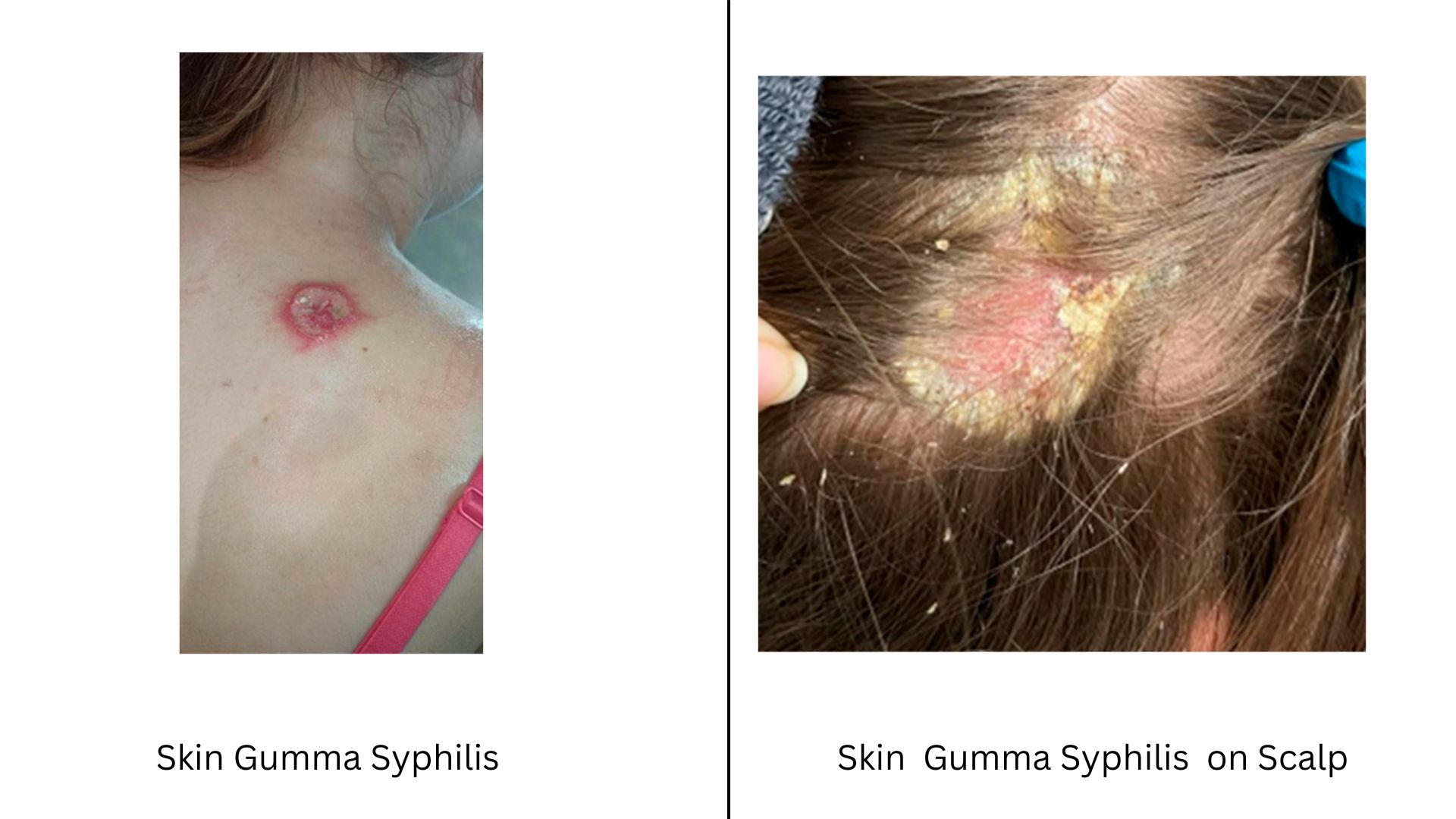
Image of Syphilis chancre on penis
{kind=link}
Image of Syphilis chancre on tongue
Image of Syphilis chancre on vagina
{kind=link}
Image of Syphilis bump on skin
Image of Syphilis ulcer over mouth
Image of Syphilis ulcer on the lips
Image of Syphilis chancre on penile shaft
{kind=link}
This sore is often firm, round, and accompanied by swollen lymph nodes in the surrounding area. Despite its innocuous appearance, the chancre teems with bacteria, making the infection highly contagious. Within 3 to 6 weeks, the sore heals spontaneously, creating a false impression of recovery. However, the bacteria have already begun spreading silently through the bloodstream and lymphatic system, setting the stage for secondary syphilis.
The Chancre’s Painless Nature: A Survival Strategy
The painlessness of the chancre is a key reason syphilis evades early detection. Unlike infections that trigger inflammation and pain, T. pallidum employs sophisticated tactics to avoid alerting the immune system. Its outer membrane lacks lipopolysaccharides (LPS), molecules that typically provoke strong inflammatory responses.
Additionally, the bacterium’s surface proteins are sparse and hidden, minimizing recognition by immune cells. Researchers also speculate that T. pallidum secretes enzymes, such as phospholipases, which may dampen pain signals and reduce local inflammation. This stealth allows the bacteria to replicate unchecked, even as the body’s immune cells gather at the infection site. The resulting ulcer is a battlefield where the immune system struggles to respond effectively, enabling the bacteria to survive and spread.
Lymph Node Involvement: A Silent Struggle
Swollen lymph nodes near the chancre reflect the body’s attempt to contain the infection. As the bacteria drain into lymphatic vessels, immune cells in the lymph nodes—such as macrophages and T cells—attempt to destroy them. However, T. pallidum’s ability to alter its surface proteins through a process called antigenic variation allows it to evade antibodies.
The tprK gene, which undergoes constant recombination, generates new protein variants, rendering previous immune responses ineffective. This genetic adaptability transforms the lymph nodes into reservoirs of infection, where the bacteria persist and multiply despite the immune system’s efforts.
Early Dissemination and Systemic Spread
Animal studies reveal that T. pallidum disseminates far earlier than previously thought. Within hours of infection, the bacteria enter the bloodstream, reaching distant organs like the brain, liver, and bones long before the chancre appears. This rapid spread is facilitated by the bacterium’s unique structure, including endoflagella that propel it through tissues. Recent research also highlights the formation of biofilm-like clusters in tissues, which protect the bacteria from antibiotics and immune attacks. These findings underscore why syphilis can progress to severe stages even after the chancre heals.
Diagnostic Challenges in Early Syphilis
Detecting primary syphilis is notoriously difficult. Blood tests, which rely on antibodies, often yield false negatives during the first 1–4 weeks because the immune system hasn’t yet produced detectable antibodies. Direct methods, such as dark-field microscopy to visualize live bacteria from chancre fluid, are more reliable but require specialized equipment.
Molecular tests like PCR, which detect bacterial DNA, offer high accuracy but are not universally available. Compounding these challenges, chancres in atypical locations (e.g., the rectum or throat) are frequently misdiagnosed as herpes, hemorrhoids, or canker sores. In individuals with HIV, delayed healing or multiple chancres further complicate diagnosis.
Coinfections and Atypical Presentations
Syphilis often coexists with other infections, particularly HIV, which alters its clinical course. HIV weakens the immune system, leading to larger or more numerous chancres that heal slowly. Conversely, syphilis increases the risk of HIV transmission by breaking down mucosal barriers. Oral or anal chancres are especially prone to misdiagnosis; for example, a painless anal ulcer might be mistaken for a fissure, delaying treatment. These complexities highlight the need for clinicians to maintain a high index of suspicion, particularly in high-risk populations.
Treatment and Prevention Strategies
Penicillin remains the gold standard for treating primary syphilis, with a single intramuscular dose effectively eliminating the infection. For penicillin-allergic patients, alternatives like doxycycline are used, though rising macrolide resistance (linked to mutations in the 23S rRNA gene) limits options like azithromycin. Prevention hinges on condom use, but since syphilis spreads via skin-to-skin contact with chancres, condoms may not fully block transmission. Regular screening is essential for sexually active individuals, especially those with multiple partners or living in high-prevalence areas. Public health efforts also emphasize partner notification and testing to break chains of transmission.
Research Frontiers: Unlocking the Bacterium’s Secrets
Scientists are unraveling how T. pallidum survives with a minimal genome—just 1.14 million base pairs and few metabolic genes. It relies entirely on the host for nutrients, a trait that complicates lab cultivation. Recent studies focus on its outer membrane proteins, which could be vaccine targets, and its ability to manipulate host immune checkpoints like PD-1, which dampen T-cell responses. Understanding these mechanisms could lead to novel therapies and improved diagnostic tools.
Secondary Syphilis: What Happens in Your Body and Why
Syphilis is a sneaky infection that can quietly spread through your body if left untreated. After the first stage (a painless sore that goes away on its own), the disease enters its secondary stage, which is like a “silent alarm” your body sounds when the infection has gone everywhere. This stage is full of confusing symptoms, from rashes to flu-like feelings, and it’s critical to understand what’s happening—and why—so you can act quickly. Let’s break it down in simple terms.
What’s Going On Inside Your Body?
When syphilis isn’t treated early, the bacteria (Treponema pallidum) don’t just stay in one place. They slip into your bloodstream and spread to your skin, organs, and even your brain. Imagine these bacteria as tiny invaders wearing invisibility cloaks. Their outer surface is slippery and hard for your immune system to detect, letting them travel undetected. Once they’ve spread, your body finally realizes something’s wrong and launches an all-out attack. But this immune response is a double-edged sword—it tries to fight the bacteria but ends up damaging your own tissues in the process.
The Symptoms: Why Do They Happen?






Image of Secondary syphilis on hands
Image of Secondary syphilis on stomach
Image of Secondary syphilis on the back
{kind=link}
Image of Secondary syphilis on the back
{kind=link}
Image of Secondary syphilis on hands
{kind=link}
Image of Secondary syphilis lesion on trunk
{kind=link}
Image of Secondary syphilis on torso
Image of Secondary syphilis on hand
Image of Secondary syphilis lesion on chest
- The Rash That Doesn’t Itch
The most common sign of secondary syphilis is a rash. Unlike allergic rashes or bug bites, this one doesn’t itch or hurt. It often starts as faint red or pink spots on your chest, back, arms, or legs. Over time, it might spread to your palms and soles. This rash is your body’s way of reacting to the bacteria hiding in your skin. Think of it like your immune system setting off fireworks to signal danger, but the bacteria are still hiding in the shadows.
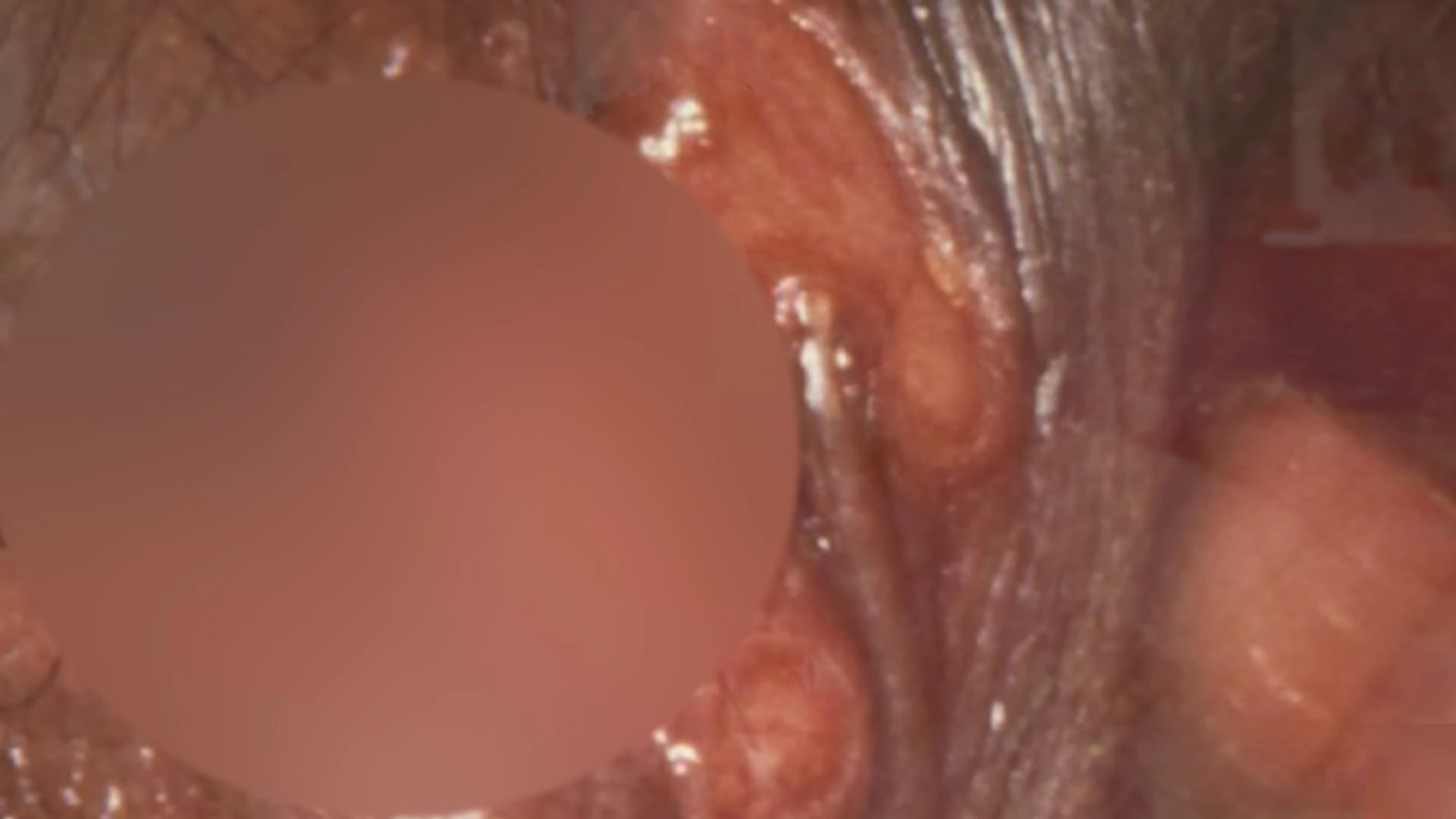
- Bumps and Sores in Moist Areas
In warm, moist places like your groin, armpits, or mouth, you might notice raised, wart-like bumps called condyloma lata. These are painless but packed with bacteria, making them highly contagious. They form because the bacteria love to nestle in areas where your skin is thin and damp.
- Flu-Like Symptoms
Feeling achy, tired, or feverish? You might chalk it up to the flu, but these are classic signs of secondary syphilis. Your body releases chemicals to fight the infection, which causes fever, headaches, and swollen lymph nodes (small glands in your neck, armpits, or groin). It’s like your immune system is yelling, “I’m working here!” but isn’t strong enough to finish the job.
- Hair Loss and Other Surprises
In rare cases, syphilis can cause patchy hair loss (like moth-eaten spots on your scalp) or eye pain and blurry vision if the bacteria reach your eyes. These symptoms happen because the infection disrupts tiny blood vessels and hair follicles.
Why Do These Symptoms Go Away on Their Own?
Here’s the tricky part: after a few weeks or months, the rash and other symptoms disappear without treatment. But this doesn’t mean the infection is gone. The bacteria are just retreating into hiding, like spies going underground. They can stay dormant for years, silently damaging your heart, brain, or nerves. This is why early treatment is so important—you don’t want to wait until the infection becomes life-threatening.
How Do Doctors Test for Secondary Syphilis?
Diagnosing this stage can be tricky because the symptoms mimic so many other illnesses. Doctors use two main tools:
- Blood Tests: These check for antibodies your body makes to fight the bacteria. However, in the early weeks, the test might miss the infection because your immune system hasn’t built up enough antibodies yet.
- Swab or Fluid Tests: If you have sores or a rash, doctors can take a sample and look for the bacteria under a special microscope or use a DNA test (PCR).
The Bigger Picture: How Syphilis Tricks Your Immune System
Scientists have discovered that Treponema pallidum is a master of disguise. It constantly changes its outer “coat” (proteins) to avoid being recognized by your immune system. Imagine a criminal changing outfits to dodge the police—this is what the bacteria do to survive. They can also form clumps (like sticky biofilms) in your tissues, making them harder to kill with antibiotics.
Another shocking fact: even during the secondary stage, the bacteria can invade your brain or spinal cord. You might not notice symptoms right away, but over time, this can lead to serious problems like memory loss or paralysis.
Treatment: How to Beat Secondary Syphilis
The good news? A simple penicillin shot can cure syphilis at this stage. If you’re allergic to penicillin, doctors can use other antibiotics like doxycycline. After treatment, you’ll need follow-up blood tests to ensure the infection is gone.
Why Treatment Matters
Without treatment, the bacteria will keep hiding in your body. Years later, they can resurface and damage your organs—a stage called tertiary syphilis, which can cause blindness, heart disease, or dementia.
Prevention: How to Stay Safe
- Use Condoms: They reduce the risk but don’t eliminate it entirely, since syphilis can spread through skin contact with sores.
- Get Tested Regularly: If you’re sexually active with multiple partners, ask for an STI screen during checkups.
- Notify Partners: If you test positive, your recent partners need testing too. This stops the infection from spreading further.
Latent Stage of Syphilis
Syphilis, caused by the spirochete Treponema pallidum, is renowned for its complex natural history and its moniker, “the great imitator,” owing to its varied clinical manifestations. Following the more overt primary and secondary stages—where patients typically develop painful chancres and rashes—the infection often enters a prolonged asymptomatic phase known as latent syphilis.
Despite the absence of overt clinical signs, the bacterium remains active within the host and can eventually lead to severe complications if untreated. Interestingly, the latent stage can persist for years or even decades, making it a silent reservoir for both reinfection and the potential progression to tertiary syphilis.
Classification of Latent Stage
Latent syphilis is defined by the presence of serologic reactivity to T. pallidum in the absence of any clinical symptoms of the disease. For epidemiologic and treatment purposes, this stage is typically subdivided into two categories:
- Early Latent Syphilis: Infection acquired within the last 12 months. Although asymptomatic, individuals in this phase may still be infectious, as up to 25% can experience a relapse into secondary symptoms.
- Late Latent Syphilis: Infection that has persisted for longer than 12 months. In this phase, the risk of sexual transmission diminishes significantly, although vertical transmission (from mother to fetus) remains a concern.
The following table summarizes the key differences:
| Parameter | Early Latent Syphilis | Late Latent Syphilis |
| Duration Since Infection | < 12 months (some definitions extend up to 2 years) | > 12 months (or ≥2 years in some classifications) |
| Infectiousness | Remains potentially infectious (risk of relapse into secondary stage) | Considerably less infectious; however, vertical transmission can occur |
| Diagnostic Criteria | Documented seroconversion or recent fourfold titer increase; history of exposure within 12 months | No recent symptoms/exposure; reactive serology with no evidence of recent infection |
| Treatment Approach | Single-dose benzathine penicillin G (2.4 million units IM) | Three weekly doses of benzathine penicillin G (2.4 million units IM each) |
Pathogenesis and Natural History
After the initial primary and secondary stages—where T. pallidum disseminates hematogenously—the infection often “disappears” from a clinical perspective, even though the organism is not eradicated from the body. In the latent phase, T. pallidum persists within tissues, particularly in areas that may be immunologically privileged. This persistence is partly attributed to its remarkable ability to evade host immune responses. One intriguing aspect of its biology is the antigenic variation of surface proteins, notably the Tpr (Treponema pallidum repeat) family. The high variability of TprK, for example, allows the spirochete to continually change its antigenic profile, thereby avoiding detection and clearance by the host’s immune system.
An interesting fact is that even though patients show no clinical symptoms during the latent stage, serologic markers (both nontreponemal and treponemal antibodies) remain positive. In some individuals, titers may decline to low levels (a phenomenon sometimes referred to as the “serofast state”), which can complicate both diagnosis and post-treatment follow-up.
Diagnosis of Latent Syphilis
Because the latent phase is clinically silent, its detection depends entirely on serologic testing. Two major categories of tests are used:
- Nontreponemal Tests (e.g., RPR, VDRL): These tests detect antibodies directed against cardiolipin-lecithin-cholesterol antigens. They are useful for screening and for monitoring treatment response, as titers generally decline after effective therapy. However, these tests are susceptible to false-negative results (such as the “prozone effect”) and may be less sensitive during the early latent phase.
- Treponemal Tests (e.g., FTA-ABS, TPPA): These assays detect antibodies that specifically target T. pallidum antigens and remain positive for life. They are used to confirm a diagnosis of syphilis after a reactive nontreponemal test.
A simplified overview of the testing strategy is provided in the table below:
| Test Type | Utility | Limitation |
| Nontreponemal Tests | Screening; monitoring treatment response (quantitative titers) | False negatives (e.g., prozone effect); titers can remain low despite treatment |
| Treponemal Tests | Confirmatory diagnosis; lifelong positivity indicates past exposure | Cannot differentiate between active and past infection; not useful for monitoring treatment efficacy |
Clinical Significance
Even though individuals with latent syphilis are asymptomatic, the stage is clinically significant for several reasons:
- Transmission Risk: Patients in the early latent phase remain capable of transmitting the infection sexually. In contrast, those in the late latent phase pose minimal sexual transmission risk but still have the potential for vertical transmission during pregnancy.
- Progression to Tertiary Syphilis: Without appropriate treatment, latent syphilis can eventually progress to tertiary syphilis, a stage characterized by severe complications such as cardiovascular damage, neurosyphilis, and gummatous lesions.
- Public Health Implications: Routine screening for syphilis, especially in high-risk populations, is crucial as many infections remain undiagnosed during this silent phase. The latent stage also presents a challenge in monitoring treatment response, particularly in patients who achieve a serofast state.
Treatment Regimens
The primary goal of treating latent syphilis is to eradicate the persistent infection and prevent progression to late-stage disease. Treatment recommendations differ based on the duration of infection:
- Early Latent Syphilis: A single intramuscular injection of benzathine penicillin G (2.4 million units) is typically recommended.
- Late Latent Syphilis: The regimen usually involves three doses of benzathine penicillin G (each 2.4 million units) administered intramuscularly at weekly intervals.
The table below outlines the standard treatment protocols:
| Stage | Treatment Regimen |
| Early Latent Syphilis | Benzathine penicillin G 2.4 million units IM, single dose |
| Late Latent Syphilis | Benzathine penicillin G 2.4 million units IM, repeated weekly for 3 weeks (total 7.2 million units) |
It is important to note that in special populations (e.g., pregnant women or HIV-infected patients), additional considerations for dosing and follow-up may be warranted.
Epidemiology and Public Health Considerations
Despite a decline in some regions due to antibiotic use and improved screening, syphilis remains a significant public health concern. Latent syphilis is frequently detected through routine screening programs, especially among individuals who are asymptomatic. Its silent nature not only poses a risk for reinfection and vertical transmission but also underscores the need for continual public health vigilance and education.
An intriguing aspect is the potential for reactivation. Although many patients remain asymptomatic for years, periodic relapses into secondary manifestations can occur, suggesting that the bacterium may periodically overcome host immune defenses even during latency.
Future Directions in Research
Research into latent syphilis is ongoing, with several areas of interest:
- Antigenic Variation: Understanding the molecular mechanisms behind the antigenic variation of Tpr proteins, particularly TprK, may open new avenues for vaccine development and therapeutic interventions.
- Immune Evasion: Further elucidation of how T. pallidum evades the immune system during latency could lead to novel diagnostic markers that distinguish between active infection, past infection, and the serofast state.
- Culture Methods: Recent advances in in vitro culture techniques, though still challenging, offer hope for more detailed studies on the bacterium’s metabolism and drug susceptibility.
Tertiary Syphilis Stage
Tertiary syphilis represents the late sequelae of untreated syphilis infection caused by Treponema pallidum. Unlike the early stages, which may resolve spontaneously with or without treatment, tertiary syphilis emerges after a long latent period—often 10 to 30 years after the initial infection—and is characterized by chronic, progressive tissue destruction. This stage is not only a marker of advanced disease but also a public health challenge since it reflects a failure in early diagnosis and treatment. The complications seen in tertiary syphilis can affect the cardiovascular system, the central nervous system, and even lead to the formation of destructive granulomatous lesions known as gummas.





Images of Tertiary Syphilis gummas leading to palatal perforation.
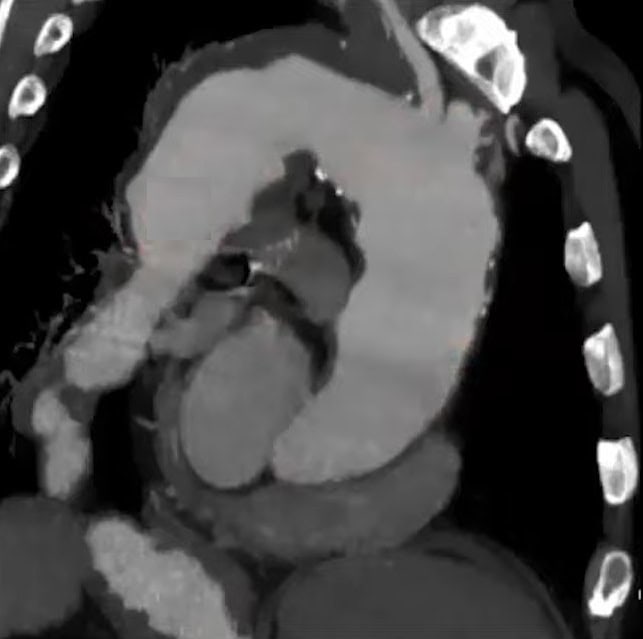
Image observed in a scan Tertiary syphilis abnormal aorta curvature
Image of Tertiary Syphilis symptoms Gummas on the leg of a patient
Image of Tertiary Syphilis stage affecting the eyes ocular optic syphilis
{kind=link}
MRI of brain of the person affected by syphilis in tertiary stage
Image of Tertiary syphilis symptom aortic aneurysm on the chest
Image of Tertiary syphilis gummas on face and nose
Tertiary syphilis is defined by the appearance of late complications in patients with a history of untreated or inadequately treated syphilis. The manifestations are classically divided into three main categories:
- Gummatous Syphilis: Involves the formation of soft, tumor-like granulomas (gummas) in the skin, bones, and internal organs.
- Cardiovascular Syphilis: Primarily affects the aorta and its branches, leading to conditions such as syphilitic aortitis, aneurysms, and aortic valve insufficiency.
- Neurosyphilis (Late Forms): Although neurosyphilis can occur at any stage, late neurosyphilis—manifesting as general paresis or tabes dorsalis—is considered a tertiary manifestation when it occurs years after the initial infection.
The table below outlines these classifications with key clinical features:
| Category | Clinical Features | Timeframe | Pathologic Findings |
| Gummatous Syphilis | Painless, rubbery nodules or plaques (gummas) that may ulcerate; can occur on skin, bones, or viscera | 10–30+ years after infection | Granulomatous inflammation with central necrosis and fibrosis |
| Cardiovascular Syphilis | Aortitis, aneurysm formation, aortic regurgitation; may present with chest pain or heart failure | 10–30+ years after infection | Inflammation and fibrosis of the aortic wall; dilatation and regurgitation |
| Late Neurosyphilis | Cognitive decline, personality changes (general paresis); sensory deficits, ataxia, lightning pains (tabes dorsalis) | 10–30+ years after infection | Demyelination, meningeal fibrosis, and vascular inflammation in CNS |
Pathogenesis and Natural History
After the initial infection, T. pallidum disseminates via the bloodstream, and the early stages (primary, secondary, and latent) often go unnoticed or are suboptimally treated. In tertiary syphilis, the bacterium—despite its low metabolic rate—persists in sequestered sites and eventually induces a chronic inflammatory response. One of the hallmarks of this stage is the host’s immune-mediated damage; as the bacterium evades immune surveillance through antigenic variation (notably of the Tpr proteins), persistent low-grade inflammation results.
Over many years, this results in the formation of gummas, inflammatory lesions that represent the body’s attempt to wall off the infection. In cardiovascular syphilis, inflammation of the vasa vasorum leads to ischemia and weakening of the aortic wall, while in neurosyphilis, chronic meningeal inflammation and subsequent parenchymal damage lead to devastating neurological deficits.
An interesting fact is that even after an effective immune response in the earlier stages, a subset of patients will progress to tertiary complications—a process that appears to be influenced by both bacterial factors (such as slow replication and immune evasion strategies) and host factors (such as age and immune status)
Clinical Manifestations
Tertiary syphilis is unique in its capacity to affect multiple organ systems. Its clinical presentation can be subtle and varied, often mimicking other chronic conditions. Key manifestations include:
Gummatous Syphilis
Gummas are soft, granulomatous lesions that can form in virtually any tissue. They are typically non-tender and may gradually enlarge before eventually ulcerating. Gummatous lesions most commonly occur on the skin and bones but can also involve visceral organs such as the liver or lungs. Although they are not infectious, their presence is a sign of extensive tissue destruction and chronic inflammation.
Cardiovascular Syphilis
Cardiovascular involvement usually targets the ascending aorta. The inflammatory process affects the vasa vasorum—small vessels that supply the aortic wall—leading to fibrosis, necrosis, and eventual dilatation. This process can culminate in syphilitic aortitis, aneurysm formation, and aortic regurgitation. Patients may present with symptoms ranging from chest pain to signs of congestive heart failure, and in some cases, sudden cardiac events may occur.
Late Neurosyphilis
While neurosyphilis can be an early complication, the late forms of neurosyphilis, such as general paresis and tabes dorsalis, typically occur decades after the initial infection. General paresis manifests with progressive cognitive impairment, personality changes, and psychiatric disturbances. Tabes dorsalis is characterized by demyelination of the posterior columns of the spinal cord, leading to sensory ataxia, lightning pains, and the classic Argyll Robertson pupil (where the pupils accommodate but do not react to bright light).
Diagnosis of Tertiary Syphilis
Diagnosing tertiary syphilis can be challenging because of its long latency and overlap with other age-related or degenerative conditions. The diagnosis primarily relies on:
- Clinical History and Examination: A detailed history of untreated or inadequately treated syphilis is crucial. Findings such as gummatous lesions, cardiovascular abnormalities on imaging, or neurological deficits in the appropriate context raise suspicion.
- Serologic Testing: Both nontreponemal tests (e.g., VDRL, RPR) and treponemal tests (e.g., FTA-ABS) remain positive in tertiary syphilis. However, while serology confirms exposure, it cannot gauge the extent of organ involvement.
- Imaging and Functional Studies: In cases of cardiovascular syphilis, echocardiography or CT/MRI imaging can reveal aortic abnormalities. Neurological evaluation, including lumbar puncture and CSF analysis, is essential when neurosyphilis is suspected.
A combined diagnostic approach is usually required, as serologic tests alone do not distinguish between latent and tertiary disease.
Treatment Strategies
Treatment of tertiary syphilis focuses on halting disease progression and preventing further organ damage. The standard treatment involves:
- Benzathine Penicillin G: For cardiovascular and gummatous syphilis, the recommended regimen is benzathine penicillin G 7.2 million units total, administered as 2.4 million units intramuscularly once a week for three consecutive weeks.
- Neurosyphilis Treatment: When neurosyphilis is present, the regimen shifts to aqueous crystalline penicillin G (18–24 million units per day administered intravenously for 10–14 days). Some experts advocate additional weekly doses of benzathine penicillin G after completing IV therapy to ensure comparable total duration of treatment.
The table below summarizes the treatment regimens for tertiary syphilis:
| Manifestation | Recommended Treatment | Route & Duration |
| Gummatous & Cardiovascular Syphilis | Benzathine penicillin G 7.2 million units total | 2.4 million units IM once weekly for 3 weeks |
| Neurosyphilis (Late Forms) | Aqueous crystalline penicillin G (preferred) | 18–24 million units/day IV for 10–14 days; followed by optional weekly IM doses |
| Alternative (Penicillin-Allergic Patients) | For non-pregnant patients, doxycycline or ceftriaxone may be considered, but penicillin remains the gold standard; desensitization is advised for pregnant women and those with neurosyphilis | Doxycycline: 100 mg orally twice daily for 28 days; however, efficacy data are limited in tertiary disease |
It is crucial to note that once irreversible damage has occurred (e.g., aortic valve damage or neurosyphilis-induced cognitive deficits), antibiotic treatment may not reverse existing pathology but can prevent further progression.
Epidemiology and Public Health Implications
Tertiary syphilis is now relatively rare in many high-income countries due to early detection and treatment. However, its presence remains an indicator of gaps in healthcare access and public health infrastructure. Outbreaks or increases in syphilis cases can eventually lead to a resurgence of tertiary complications if screening and treatment programs are not maintained. Moreover, tertiary syphilis has significant morbidity, with long-term disability resulting from cardiovascular and neurological damage, which poses challenges for health systems.
An interesting public health fact is that while the overall incidence of syphilis has increased in some populations in recent years, the majority of cases are still detected and managed in the earlier stages. Nonetheless, tertiary syphilis serves as a stark reminder of the long-term consequences of untreated sexually transmitted infections
Future Directions in Research
Current research efforts aim to:
- Elucidate Molecular Mechanisms: Studies continue to investigate the host-pathogen interactions and immune evasion strategies of T. pallidum, including how persistent infection leads to tissue destruction in tertiary syphilis.
- Improve Diagnostic Modalities: Advanced imaging techniques and novel biomarkers are being explored to differentiate tertiary syphilis from other chronic diseases.
- Optimize Treatment Regimens: Research is underway to determine whether prolonged or combination antibiotic regimens might improve outcomes in patients with late-stage neurosyphilis or cardiovascular involvement.
Vaccine Development: Despite the formidable challenges posed by antigenic variation and the bacterium’s stealth properties, efforts to develop a vaccine remain an important long-term goal.
Conclusion
The primary stage of syphilis, though seemingly mild, is a crucial period where early detection and treatment can prevent severe complications. The painless chancre and subtle systemic spread make this infection deceptive, often allowing it to advance unnoticed. Understanding the mechanisms behind syphilis, from immune evasion to bacterial dissemination, empowers individuals to recognize symptoms early and seek timely intervention. Given the high success rate of treatment with antibiotics like penicillin, proactive testing and awareness remain the best defenses against this silent threat.
For those at risk, routine screenings and safe practices are essential to curbing syphilis transmission. If you suspect exposure or notice any concerning signs, consult a healthcare provider promptly. Addressing syphilis in its earliest stage not only safeguards personal health but also plays a vital role in controlling its spread within communities.


References
- General information on syphilis: www.generalsource.com
- Bacterial mechanisms and immune evasion: www.microbiologytextbook.com
- Syphilis diagnostic guidelines: www.healthguidelines.org
- Epidemiological data and public health strategies: www.stddatareport.com
- Medical treatment protocols: www.medicalreferencepage.com
For specific medical concerns, always consult a qualified healthcare provider.